
Otitis Media with Effusion (OME)
What is otitis media with effusion (OME)?
Otitis media with effusion (OME) is a collection of non-infected fluid in the middle ear space. It is also called serous or secretory otitis media (SOM). This fluid may accumulate in the middle ear as a result of a cold, sore throat or upper respiratory infection.
OME is usually self-limited, which means, the fluid usually resolves on its own within 4 to 6 weeks. However, in some instances the fluid may persist for a longer period of time and cause a temporary decrease in hearing or the fluid may become infected (acute otitis media).
OME is more common in children between 6 months and 3 years of age, and affects more boys than girls. The condition occurs more often in the fall and winter months and is commonly underdiagnosed because of its lack of acute or obvious symptoms (compared to acute otitis media (AOM).
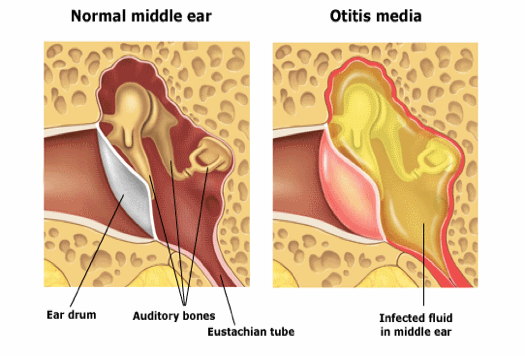
ASOM (Acute Suppurative Otitis Media)
In the United States, acute otitis media (AOM), defined by convention as the first 3 weeks of a process in which the middle ear shows the signs and symptoms of acute inflammation, is the most common affliction necessitating medical therapy for children younger than 5 years. [1, 2, 37] See the image below.

Tympanic membrane of a person with 12 hours of ear pain, slight tympanic membrane bulge, and slight meniscus of purulent effusion at bottom of tympanic membrane.
Signs and symptoms
Although the history of AOM varies with age, a number of constant features manifest during the otitis-prone years, including the following:
Neonates: Irritability or feeding difficulties may be the only indication of a septic focus
Older children: This age group begins to demonstrate a consistent presence of fever and otalgia, or ear tugging
Older children and adults: Hearing loss becomes a constant feature of AOM and otitis media with effusion (OME); ear stuffiness is noted before the detection of middle ear fluid
Ear pain without hearing loss or fever is observed in adults with external otitis media, dental abscess, or pain referred from the temporomandibular joint. Orthodontic appliances often elicit referred pain as the dental occlusion is altered. Diagnosis
Pneumatic otoscopy is the standard of care in the diagnosis of acute and chronic otitis media. The following findings may be found on examination in patients with AOM:
- Signs of inflammation in the tympanic membrane
- Bulging in the posterior quadrants of the tympanic membrane may bulge; scalded appearance of the superficial epithelial layer
- Perforated tympanic membrane (most frequently in posterior or inferior quadrants)
- Presence of an opaque serumlike exudate oozing through the entire tympanic membrane
- Pain with/without pulsation of the otorrhea
- Fever
Testing
Testing in the acute phase is generally unhelpful, because all children with AOM have conductive hearing loss associated with the middle ear effusion. In addition, although tympanometry may assist in the diagnosis of middle ear effusion, this test is seldom necessary for the skilled pneumatic otoscopist.
Culture and sensitivity of a specimen from a fresh perforation or a tympanocentesis may be helpful. Imaging studies
Radiologic studies are generally unnecessary in uncomplicated AOM. However, CT scanning may be necessary to determine if a complication has occurred. MRI might be more appropriate for diagnosing suspected intracranial complications.
Procedure
No surgical procedures are required in majority of the cases of ASOM. However, Tympanocentesis i.e. aspiration of the contents of the middle ear cleft by piercing the tympanic membrane with a needle and collecting that material for diagnostic examination can be offered in some select cases. E.g.
- Neonates who are younger than 6 weeks (and therefore are more likely to have an unusual or more invasive pathogen)
- Immunosuppressed or immunocompromised patients
- Patients in whom adequate antimicrobial treatment has failed and who continue to show signs of local or systemic sepsis
- Patients with a complication that requires a culture for adequate therapy
Management
Pharmacotherapy
Antibiotics are the only medications with demonstrated efficacy in the management of AOM; therefore, these agents are the initial therapy of choice. The antibiotic chosen should cover most of the common bacterial pathogens and be individualized for the child with regard to allergy, tolerance, and previous exposure to antibiotics, cost, and community resistance levels. Duration of treatment may also be a consideration in the choice of antibiotic.
Common antibiotics used in the management of AOM include the following:
- Amoxicillin
- Amoxicillin/clavulanate
- Erythromycin base/sulfisoxazole
- Trimethoprim-sulfamethoxazole
- Cefixime
- Cefuroxime axetil
- Cefprozil
- Cefpodoxime
- Cefdinir
- Clindamycin
- Clarithromycin
- Azithromycin
- Ceftriaxone
Surgery ( rarely required)
Surgical management of AOM can be divided into the following 3 related procedures:
- Tympanocentesis
- Myringotomy
- Myringotomy with insertion of a ventilating tube
Selection of the appropriate procedure results from evaluation of patient factors, surgeon factors, available resources, and urgency.
Chronic Suppurative Otitis Media
What is chronic suppurative otitis media?
Chronic suppurative otitis media is chronic infection in part or whole of the middle ear cleft.
What are the different types of chronic suppurative otitis media (CSOM)?
1. Tubotympanic type: (safe type)
Causes:
Usually sequelae of acute otitis media infection, leaving behind a perforation. Recurrent infections via the eustachian tube (tube connecting Middle ear with back of Nose: nasopharynx) commonly from the tonsils or adenoids Traumatic perforation.
Clinical features:
- Perforation: It is usually a central perforation with a safe margin of healthy remanant tympanic membrane around it in the pars tensa.
- Hearing loss: It is a purely conductive type of hearing loss, rarely exceeding 40-45 db.
- Discharge: It is mucoid, copious, non-foul smelling and is related to a bout of upper respiratory tract infection.
- A quiescent phase in the ear symptoms may be present.
2. Atticoantral type: (unsafe type)
It involves the posterio-superior part of the middle ear cleft and is usually associated with cholesteatoma. Aetiology:
- Congenital: These are squamous epithelial cell nests arising within the temporal bone.
- Acquired:
- Primary: Develops in continuity with the pars flacida of the tympanic membrane
- Secondary: This can occur by:
- Immigration of the tympanic membrane epithelium
- Metaplasia: Middle ear mucosa undergoes metaplasia due to repeated infections.
- Negative middle ear pressure.
Clinical features:
- Perforation: It is usually in attic region, postero-superior region, or marginal.
- Retraction pocket: A retraction or invagination of the tympanic membrane is seen in attic or postero-superior region of pars tensa
- Cholesteatoma: This can be seen in the form of pearly white flakes.
What are the investigations required to confirm the diagnosis of chronic suppurative otitis media (CSOM)?
- Suction Microscopy: To suck out any discharge, confirm clinical findings and examination of the discharge for pus culture and antibiotic sensitivity.
- Tuning fork tests: They help in clinical evaluation of hearing loss.
- Pure tone audiogram: This is useful for a qualitative and quantitative analysis of the patients hearing. It also helps for pre-operative and post operative assessment of the hearing loss and for medico-legal purposes.
- X-ray mastoid Schuller’s view: To diagnose the extent of disease and status of the mastoid air cells
- Routine blood investigations from fitness point of view.
- High resolution CT scan of the temporal bone is extremely useful in patients with complications or impending complications.
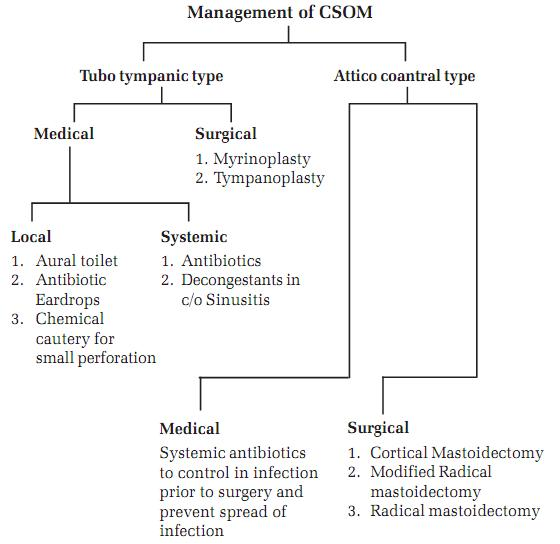
What is the treatment for chronic suppurative otitis media (CSOM)?
1) Tubotympanic type
A) Medical:
- Local
- Aural toilet
- Antibiotic ear drops
- Chemical cautery for small perforations
- Systemic
- Antibiotics
- Decongestant in case of sinusitis.
- Antioxidants
B) Surgical
- Myringoplasty
- Tympanoplasty with or without a mastoidectomy.
2) Atticoantral Type:
A) Medical:
- Systemic antibiotics to control the infection prior to surgery and prevent spread of infection.
- Medical line of treatment has limited role in unsafe CSOM.
B) Surgical:
- Cortical mastoidectomy
- Modified radical mastoidectomy
- Radical mastoidectomy.
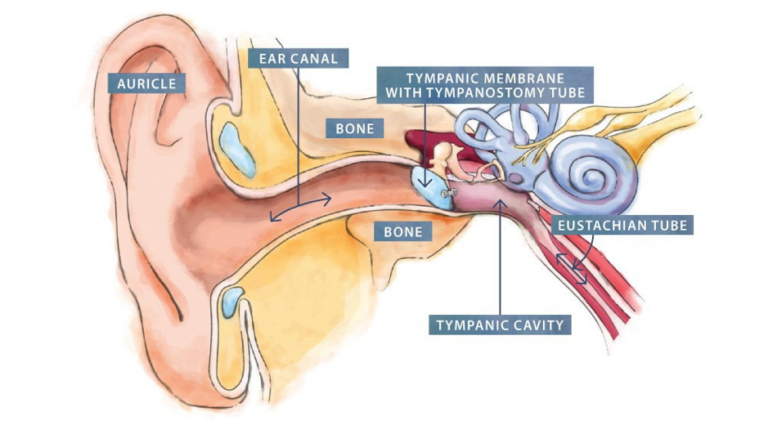
Otitis Externa
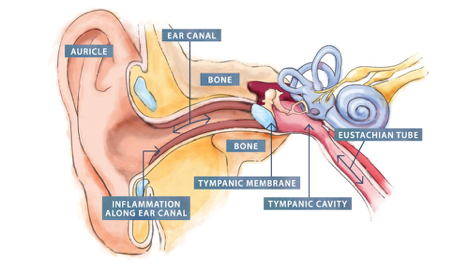
Otitis externa is a condition that causes inflammation (redness and swelling) of the external ear canal, which is the tube between the outer ear and eardrum.
Otitis externa is often referred to as “swimmer’s ear” because repeated exposure to water can make the ear canal more vulnerable to inflammation.
Symptoms of otitis externa include:
- ear pain, which can be severe
- itchiness in the ear canal
- a discharge of liquid or pus from the ear
- some degree of temporary hearing loss
Usually only one ear is affected.
With treatment, these symptoms should clear up within a few days. However, some cases can persist for several months or longer
When to see your Doctor
You should see your Doctor if you may have otitis externa.
Your Doctor will ask about your symptoms and whether you regularly use any items that are inserted into your ears, such as hearing aids or ear plugs. They may also examine inside your ear using an instrument called an otoscope.
If you have recurring episodes of otitis externa that haven’t responded to treatment, your Doctor may take a swab of the inside of your ear. This will be tested to help determine what type of infection you have, if any, so appropriate medication can be prescribed.
What causes otitis externa?
Most cases of otitis externa are caused by a bacterial infection, although the condition can also be caused by:
- irritation
- fungal infections
- allergies
There are a number of things that can make you more likely to develop otitis externa, including:
- damaging the skin inside your ear
- regularly getting water in your ear
Getting water in your ear is particularly significant, because this can cause you to scratch inside your ear, and the moisture also provides an ideal environment for bacteria to grow.
Who is affected?
Otitis externa is relatively common. It’s estimated that around 1 in 10 people will be affected by it at some point in their lives. The condition is slightly more common in women than men and is most often diagnosed in adults aged 45 to 75.
People with certain long-term (chronic) conditions are at greater risk of developing the condition. These include:
- eczema
- asthma
- allergic rhinitis
How otitis externa is treated
Otitis externa sometimes gets better without treatment, but it can take several weeks. Your Doctor can prescribe ear drop medication that usually improves the symptoms within a few days. There are a number of different types of ear drops that may be used to treat otitis externa, but they all tend to be used several times a day for about a week.
Your Doctor may refer you to a specialist for further treatment and advice if symptoms are severe or they fail to respond to treatment. Preventing otitis externa
To help reduce your chances of developing otitis externa, you should avoid inserting cotton wool buds and other things into your ears (including your fingers), as this can damage the sensitive skin in your ear canal.
If you’re a regular swimmer, consider using ear plugs when swimming or wearing a swimming cap to cover your ears and protect them from water.
You should also try to avoid getting water, soap or shampoo into your ears when you have a shower or bath.
Complications
Complications of otitis externa are uncommon, but some can be very serious.
One rare complication of otitis externa is malignant otitis externa, which is where an infection spreads from the ear canal into the surrounding bone. This variety is common in diabetics & patients with low immunity (immuno-compromised).
This requires prompt treatment with antibiotics and sometimes surgery, as it can be fatal if left untreated.
Ear Wax
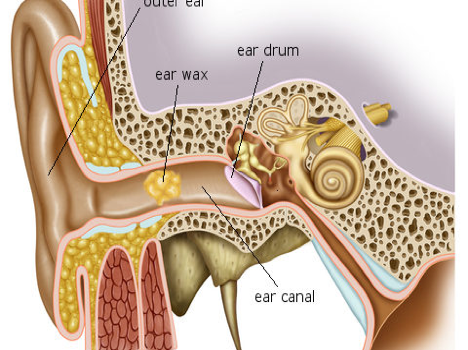
Good intentions to keep ears clean may weaken the ability to hear. The ear is a delicate and intricate body part, including the skin of the ear canal and the eardrum. Therefore, special care should be given to this part of the body. Start by discontinuing the habit of inserting cotton-tipped applicators or other objects into the ear canals.
WHY DOES THE BODY PRODUCE EARWAX?
Cerumen or earwax is healthy in normal amounts and serves as a self-cleaning agent with protective, lubricating, and antibacterial properties. The absence of earwax may result in dry, itchy ears. Self-cleaning means there is a slow and orderly movement of earwax and dead skin cells from the eardrum to the ear opening. Old earwax is constantly being transported, assisted by chewing and jaw motion, from the ear canal to the ear opening where, most of the time, it dries, flakes, and falls out.
Earwax is not formed in the deep part of the ear canal near the eardrum. It is only formed in the outer one-third of the ear canal. So, when a patient has wax blockage against the eardrum, it is often because he has been probing the ear with such things as cotton-tipped applicators, bobby pins, or twisted napkin corners. These objects only push the wax in deeper.
WHEN SHOULD THE EARS BE CLEANED?
Under ideal circumstances, the ear canals should never have to be cleaned. However, that isn’t always the case. The ears should be cleaned when enough earwax accumulates to cause symptoms or to prevent a needed assessment of the ear by your doctor. This condition is call cerumen impaction, and may cause one or more of the following symptoms:
- Earache, fullness in the ear, or a sensation the ear is plugged
- Partial hearing loss, which may be progressive
- Tinnitus, ringing, or noises in the ear
- Itching, odor, or discharge
- Coughing
WHAT IS THE RECOMMENDED METHOD OF EAR CLEANING?
Ideally, ear wax does not need to be cleaned, in fact they offer protection to the skin of outer ear canal from variety of bacterial and fungal infections. They serve similar functions as saliva in mouth or tear in our eyes. However, when the accumulation of ear wax is significant enough to cause hearing loss, Tinnitus or the doctor is unable to have a good view of the ear drums, they can be removed under direct vison by a trained ENT surgeon.
Irrigation or ear syringing is commonly used for cleaning and can be performed by a ENT physician using a commercially available irrigation kit. Common solutions used for syringing include water and saline, which should be warmed to body temperature to prevent dizziness. Ear syringing is most effective when water, saline, or wax dissolving drops are put in the ear canal 15 to 30 minutes before treatment. Caution is advised to avoid having your ears irrigated if you have diabetes, a hole in the eardrum (perforation), tube in the eardrum, skin problems such as eczema in the ear canal or a weakened immune system.
Manual removal of earwax is also effective. This is most often performed by an ENT doctor using suction or special miniature instruments, and a microscope to magnify the ear canal. Manual removal is preferred if your ear canal is narrow, the eardrum has a perforation or tube, other methods have failed, or if you have skin problems affecting the ear canal, diabetes or a weakened immune system.
WHY SHOULDN’T COTTON SWABS BE USED TO CLEAN EARWAX?
Wax blockage is one of the most common causes of hearing loss. This is often caused by attempts to clean the ear with cotton swabs. Most cleaning attempts merely push the wax deeper into the ear canal, causing a blockage.
The outer Ear is the funnel-like part of the ear that can be seen on the side of the head, plus the ear canal (the hole which leads down to the eardrum). The ear canal is shaped somewhat like an hourglass narrowing part way down. The skin of the outer part of the canal has special glands that produce earwax. This wax is supposed to trap dust and dirt particles to keep them from reaching the eardrum. Usually the wax accumulates a bit, dries out, and then comes out of the ear, carrying dirt and dust with it. Or it may slowly migrate to the outside where it can be wiped off.
ARE EAR CANDLES AN OPTION FOR REMOVING WAX BUILD UP?
No, ear candles are not a safe option of wax removal as they may result in serious injury. Since users are instructed to insert the 10- to 15-inch-long, cone-shaped, hollow candles, typically made of wax-impregnated cloth, into the ear canal and light the exposed end, some of the most common injuries are burns, obstruction of the ear canal with wax of the candle, or perforation of the membrane that separates the ear canal and the middle ear.
The U.S. Food and Drug Administration (FDA) became concerned about the safety issues with ear candles after receiving reports of patient injury caused by the ear candling procedure. There are no controlled studies or other scientific evidence that support the safety and effectiveness of these devices for any of the purported claims or intended uses as contained in the labelling.
WHEN SHOULD A DOCTOR BE CONSULTED?
If the home treatments discussed in this leaflet are not satisfactory or if wax has accumulated so much that it blocks the ear canal (and hearing), a physician may prescribe eardrops designed to soften wax, or she may wash or vacuum it out. Occasionally, an otolaryngologist (ear, nose, and throat specialist) may need to remove the wax under microscopic visualization. If there is a possibility of a perforation in the eardrum, consult a physician prior to trying any over-the-counter remedies. Putting eardrops or other products in the ear with the presence of an eardrum perforation may cause pain or an infection. Certainly, washing water through such a hole could start an infection.
WHAT CAN I DO TO PREVENT EXCESSIVE EARWAX?
There are no proven ways to prevent cerumen impaction, but not inserting cotton-tipped swabs or other objects in the ear canal is strongly advised. If you are prone to repeated wax impaction or use hearing aids, consider seeing your doctor every 6 to 12 months for a checkup and routine preventive cleaning.
What is otosclerosis?
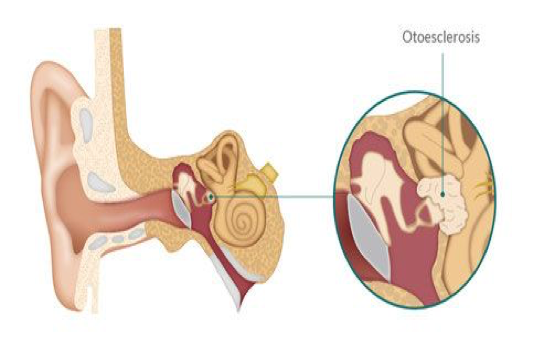
Otosclerosis is a hereditary condition that causes the abnormal growth of bone of the middle ear and inner ear. This bone prevents structures within the ear from working properly and causes hearing loss. For some people with otosclerosis, the hearing loss may become severe.
How does Otosclerosis cause hearing impairment?
Otosclerosis can cause different types of hearing loss, depending on which structure within the ear is affected. Otosclerosis usually affects the last bone in the chain, the stapes, which rests in the entrance to the inner ear (the oval window). The abnormal bone fixates the stapes in the oval window and interferes with sound passing waves to the inner ear. This causes a conductive or mechanical hearing loss, a hearing loss caused by a problem in the outer or middle ear. Less frequently, otosclerosis may cause a sensorineural hearing loss (damaged sensory cells and/or nerve fibers of the inner ear). Most patients with Otosclerosis have a combination of these problems, or a mixed hearing loss. Next commonly, patients may have a pure conductive hearing loss. The least common pattern is a sensorineural pattern which can sometimes be difficult to diagnose as it can mimic hearing loss from other causes. Otolsclerosis may cause mild to profound hearing loss and is very variable amongst those affected.
What causes Otosclerosis?
The cause of otosclerosis is not fully understood, although it is a hereditary problem, or passed down from parent to child. Many different genes seem to be involved in this problem. It can skip generations and be silent and appear to cause hearing loss in a person without a known family history of it. It can cause different severities of hearing loss amongst those affected in the family. It may be completely silent in one person, but be passed on through genetics to their children.
People who have a family history of otosclerosis are more likely to develop the disorder. On average, a person who has one parent with otosclerosis has a 25 percent chance of developing the disorder. If both parents have otosclerosis, the risk goes up to 50 percent. Research shows that white, middle-aged women are most at risk.
Some research suggests a relationship between otosclerosis and the hormonal changes associated with pregnancy. While the exact cause remains unknown, there is some evidence associating viral infections (such as measles) and otosclerosis.
What are the symptoms of otosclerosis?
Hearing loss is the most frequent symptom of otosclerosis. The loss may appear very gradually. Many people with otosclerosis first notice that they cannot hear low-pitched sounds or that they can no longer hear a whisper. In addition to hearing loss, some people with otosclerosis may experience dizziness, balance problems, or tinnitus. Tinnitus is a sensation of ringing, roaring, buzzing, or hissing in the ears or head that accompanies many forms of hearing loss.
How is otosclerosis diagnosed?
Otosclerosis is diagnosed by a careful physical examination and audiolocal testing. The acoustic reflex tests in the immitence part of the hearing evaluation are particularly important to it’s diagnosis. Sometimes the diagnosis takes a few years to establish, with serial audiograms being required when the hearing loss is mild, or the sensorinerual kind of hearing loss is present. A CT scan is occasionally used to confirm its presence.
How is otosclerosis treated?
Medical therapy is sometimes recommended. Fluoride therapy is thought to potentially prevent the development of sensorinerual hearing loss, but will not improve hearing loss that has already developed. Hearing aids are commonly prescribed for patients with otosclerosis. A hearing aid is designed to compensate for a hearing loss by amplifying sound. An audiologist can discuss the various types of hearing aids available and make a recommendation based on the specific needs of an individual.
Surgery is an option for treatment of the conductive or mechanical hearing loss caused by otosclerosis. In an operation called a stapedectomy, or stapedotomy, an otologist (ear surgeon) bypasses the diseased bone with a prosthetic device that allows sound waves to be passed to the inner ear. It is important to discuss the risks and possible complications of this procedure, as well as the benefits, with the surgeon. In rare cases, surgery can worsen the hearing loss.
Stapedectomy/Stapedotomy
A stapes operation can be performed to improve hearing in patients who have a “frozen” or “stuck” stapes bone. This usually occurs in patients who have the condition called otosclerosis, but can occur in other hereditary conditions or in patients who have had very severe middle ear infections or previous surgeries. The stapes is the last hearing bone in the chain of bones in the middle ear, and it is normally mobile and attached by a ligament to an opening of the bone that houses the inner ear, called the oval window. A frozen stapes bone causes a mechanical or conductive hearing loss.
The operation to allow sound to pass into the inner ear again is called a stapedectomy, or stapedotomy, depending on the size of hole made into the oval window, but the operations are pretty much the same. The surgery is usually performed on an out-patient basis and takes about an hour. It is usually performed with sedation, although some patients require general anesthesia. In most cases, the operation can be completed by working through the ear canal, although sometimes an incision needs to be made behind the ear if the ear canal is small or the anatomy is different. A microscope and laser are used.
The ear is completely numbed and incisions are made in the ear canal and the drum is lifted up out of the way. The diagnosis is confirmed by making sure that the other bones are normal. A vein graft from the hand or arm or a tissue graft from behind the ear is obtained through a tiny incision. The top of the stapes bone is removed and an opening is made into the base, or footplate of the stapes bone. A prosthesis made of titanium is placed between the hole and the incus bone and a tissue graft is used to help seal the hole. The drum is put down into position, the hearing is tested and packing is placed in the ear canal.
Post-op Care
After surgery, the patient stays in bed in the hospital for a few hours to prevent nausea and vomiting. The nurses then help the patient get up and walk and if there is no significant dizziness or nausea, the patient can be discharged home.
The patient’s activity is fairly restricted for the first week, and then a gradual return to activity can occur, but heavy exercise, staining, blowing the nose, or lifting anything more than 10 pounds needs to be avoided for 4-6 weeks. The packing is removed in the office one week after surgery and the hearing gradually returns over the next month. Water needs to be kept out of the ear for 2-3 weeks.
Complications
- Nausea and dizziness: this is common and expected after surgery and is usually mild and short lived. Many medications are given to prevent these and only a few patients feel dizzy beyond the day of surgery. Some patients feel sensitive to motion for a few days. Driving is restricted until this resolves, usually no more than a few days. If severe dizziness occurs, the patient is kept in hospital and given medication until it resolves
- Temporary change in taste: A nerve of taste runs under the ear drum and has to be moved out of the way during surgery. This can leave a loss of taste, or taste change on the side of the tongue which is usually temporary.
- No improvement in the hearing, or lack of significant improvement can occur in 2% of cases.
- High frequency hearing loss can occur in 5-10% but the improvement in other frequencies usually makes up for this.
- Tinnitus usually improves with hearing improvement after surgery, but in rare cases can occur or worsen.
- A perforated eardrum or damage to the other ear bones are rare.
- Facial nerve paralysis is extremely rare.
- Total loss of hearing can occur in 1% of cases. If this occurs, a conventional hearing aid would not help restore the hearing loss.
- Some patients develop a recurrence of hearing loss and need to undergo repeat surgery in the future. This probably happens in 5% of patients over their lifetime.
Giddiness due to Benign paroxysmal positional vertigo (BPPV)
Benign paroxysmal positional vertigo (BPPV) is one of the most common causes of vertigo — the sudden sensation that you’re spinning or that the inside of your head is spinning.
Benign paroxysmal positional vertigo causes brief episodes of mild to intense dizziness. Benign paroxysmal positional vertigo is usually triggered by specific changes in the position of your head. This might occur when you tip your head up or down, when you lie down, or when you turn over or sit up in bed.
Although benign paroxysmal positional vertigo can be a bothersome problem, it’s rarely serious except when it increases the chance of falls. You can receive effective treatment for benign paroxysmal positional vertigo during a doctor’s office visit.
Symptoms
The signs and symptoms of benign paroxysmal positional vertigo (BPPV) may include:
- Dizziness
- A sense that you or your surroundings are spinning or moving (vertigo)
- A loss of balance or unsteadiness
- Nausea
- Vomiting
The signs and symptoms of BPPV can come and go, with symptoms commonly lasting less than one minute. Episodes of benign paroxysmal positional vertigo can disappear for some time and then recur.
Activities that bring about the signs and symptoms of BPPV can vary from person to person, but are almost always brought on by a change in the position of your head. Some people also feel out of balance when standing or walking.
Abnormal rhythmic eye movements (nystagmus) usually accompany the symptoms of benign paroxysmal positional vertigo.
When to see a doctor
Generally, see your doctor if you experience any unexplained dizziness or vertigo that recurs periodically for more than one week.
Seek emergency care
Although it’s uncommon for dizziness to signal a serious illness, see your doctor immediately if you experience dizziness or vertigo along with any of the following:
- A new, different or severe headache
- A fever
- Double vision or loss of vision
- Hearing loss
- Trouble speaking
- Leg or arm weakness
- Loss of consciousness
- Falling or difficulty walking
- Numbness or tingling
The signs and symptoms listed above may signal a more serious problem.
Causes
- Often, there’s no known cause for BPPV. This is called idiopathic BPPV.
When a cause can be determined, BPPV is often associated with a minor to severe blow to your head. Less common causes of BPPV include disorders that damage your inner ear or, rarely, damage that occurs during ear surgery or during prolonged positioning on your back, such as in a dentist chair. BPPV also has been associated with migraines.
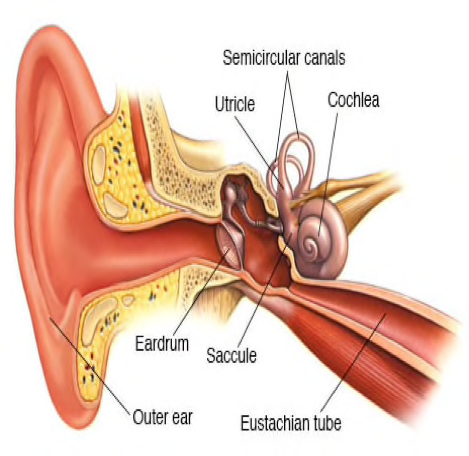
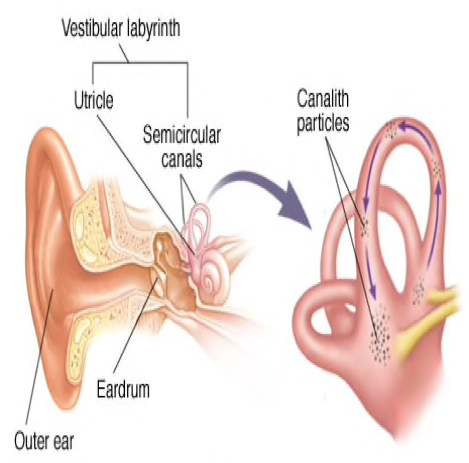
The ear’s role
Inside your ear is a tiny organ called the vestibular labyrinth. It includes three loop-shaped structures (semicircular canals) that contain fluid and fine, hair-like sensors that monitor the rotation of your head.
Other structures (otolith organs) in your ear monitor movements of your head — up and down, right and left, back and forth — and your head’s position related to gravity. These otolith organs contain crystals that make you sensitive to gravity.
For a variety of reasons, these crystals can become dislodged. When they become dislodged, they can move into one of the semicircular canals — especially while you’re lying down. This causes the semicircular canal to become sensitive to head position changes it would normally not respond to, which is what makes you feel dizzy.
Risk factors
Benign paroxysmal positional vertigo occurs most often in people age 50 and older, but can occur at any age. Benign paroxysmal positional vertigo is also more common in women than in men. A head injury or any other disorder of the balance organs of your ear may make you more susceptible to BPPV.
Complications
Although benign paroxysmal positional vertigo (BPPV) is uncomfortable, it rarely causes complications. The dizziness of BPPV can make you unsteady, which may put you at greater risk of falling.
Diagnosis
Your doctor may do a series of tests to determine the cause of your dizziness. During a physical examination, your doctor will likely look for:
- Signs and symptoms of dizziness that are prompted by eye or head movements and then decrease in less than one minute
- Dizziness with specific eye movements that occur when you lie on your back with your head turned to one side and tipped slightly over the edge of the examination bed
- Involuntary movements of your eyes from side to side (nystagmus)
- Inability to control your eye movements
If the cause of your signs and symptoms is difficult to determine, your doctor may order additional testing, such as:
- Electronystagmography (ENG) or videonystagmography (VNG). The purpose of these tests is to detect abnormal eye movement. ENG (which uses electrodes) or VNG (which uses small cameras) can help determine if dizziness is due to inner ear disease by measuring involuntary eye movements while your head is placed in different positions or your balance organs are stimulated with water or air.
- Magnetic resonance imaging (MRI). This test uses a magnetic field and radio waves to create cross-sectional images of your head and body. Your doctor can use these images to identify and diagnose a range of conditions. MRI may be performed to rule out other possible causes of vertigo.
Treatment
- The inner ear and canalith repositioning
Benign paroxysmal positional vertigo may go away on its own within a few weeks or months. But, to help relieve BPPV sooner, your doctor, audiologist or physical therapist may treat you with a series of movements known as the canalith repositioning procedure.
Canalith repositioning
Performed in your doctor’s office, the canalith repositioning procedure consists of several simple and slow maneuvers for positioning your head. The goal is to move particles from the fluid-filled semicircular canals of your inner ear into a tiny bag-like open area (vestibule) that houses one of the otolith organs in your ear where these particles don’t cause trouble and are more easily resorbed.
Each position is held for about 30 seconds after any symptoms or abnormal eye movements stop. This procedure is usually effective after one or two treatments.
Your doctor will likely teach you how to perform the canalith repositioning procedure on yourself so that you can do it at home if necessary.
Surgical alternative
In very rare situations in which the canalith repositioning procedure isn’t effective, your doctor may recommend a surgical procedure in which a bone plug is used to block the portion of your inner ear that’s causing dizziness. The plug prevents the semicircular canal in your ear from being able to respond to particle movements or head movements in general. The success rate for canal plugging surgery is approximately 90 percent.
Lifestyle and home remedies
If you experience dizziness associated with benign paroxysmal positional vertigo (BPPV), consider these tips:
- Be aware of the possibility of losing your balance, which can lead to falling and serious injury.
- Sit down immediately when you feel dizzy.
- Use good lighting if you get up at night.
- Walk with a cane for stability if you’re at risk of falling.
- Work closely with your doctor to manage your symptoms effectively.
BPPV may recur even after successful therapy. Fortunately, although there’s no cure, the condition can be managed with physical therapy and home treatments.
Preparing for your appointment
Make an appointment with your doctor if you have symptoms common to BPPV. After an initial examination, your doctor may refer you to an ear, nose and throat (ENT) specialist or a doctor who specializes in the brain and nervous system (neurologist). Here’s some information to help you get ready for your appointment.
What you can do
- Write down your symptoms, including when they started and how often they occur.
- Note any recent blows to your head, including even minor accidents or injuries.
- Make a list of your key medical information, including any other conditions for which you’re being treated and the names of any medications, vitamins and supplements you’re taking.
- Write down questions to ask your doctor. Creating your list of questions can help you make the most of your time with your doctor.